Regional Trends in Suicide Rate Statistics
What Suicide Rate Statistics Mean
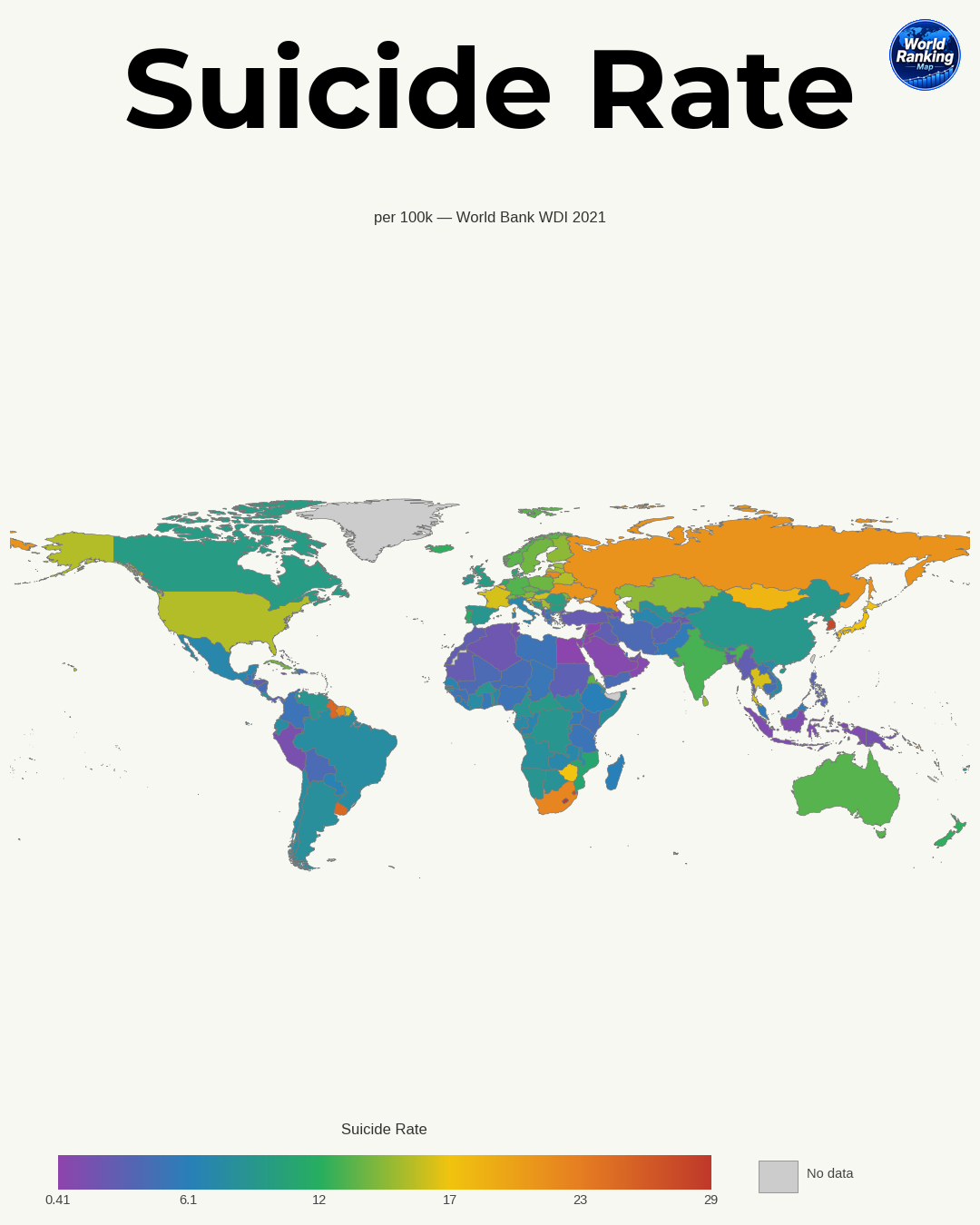
Suicide rate statistics are indicators that quantify the number of suicide deaths occurring within a specific population over a given period. They are generally expressed as the number of suicide deaths per 100,000 people and are widely used for cross-country comparisons and long-term trend analysis. Because raw death counts alone make it difficult to compare countries with large and small populations fairly, suicide rates are calculated as a proportion of the population.
When interpreting suicide rates, it is important to understand the difference between the crude suicide rate and the age-standardized suicide rate. The crude rate is calculated based on the total population, while the age-standardized rate adjusts for differences in age structure across countries. Countries with a larger older population may appear to have relatively higher suicide rates, so age-standardized figures are often more appropriate for international comparisons.
Suicide rate statistics should also be understood not simply as a numerical measure of individual choice, but as the result of a range of social conditions, including mental health, economic circumstances, family structure, social isolation, and access to healthcare. For that reason, it is important to read the background and context behind the numbers, not just the numbers themselves.
Overall Global Trends in Suicide Rates
Over the past several decades, global suicide rates have shown a gradual downward trend overall. According to the World Health Organization (WHO) and international health statistics, many countries have seen average suicide rates decline as policies such as improved mental health awareness, expanded crisis intervention services, and restrictions on access to lethal means have been implemented.
However, this decline has not been uniform across all regions. Some countries have shown a clear downward trend, while others have remained flat or even seen increases in certain age or gender groups. In particular, shocks such as economic crises, war, pandemics, rising unemployment, and social disconnection can raise suicide risk in the short term.
Common patterns often seen in international comparisons include the following:
- Men often have higher suicide rates than women
- Many countries show relatively higher rates among older adults or middle-aged people
- High-income countries do not necessarily have low suicide rates
- Countries with more sophisticated reporting systems may record higher rates more accurately
In other words, the global average alone cannot fully explain reality, and regional and national differences must also be examined.
Suicide Rate Trends in Asia
Asia is a region with a very large population and highly diverse social and economic conditions, so regional differences in suicide rates are especially pronounced. East Asia, Southeast Asia, South Asia, and Central Asia each show different patterns.
In East Asia, countries such as South Korea and Japan have long treated suicide as an important public health issue. In this region, industrialization, competitive education and work environments, aging populations, the rise of single-person households, and social isolation are often discussed as background factors. However, in recent years, some countries have also seen suicide rates fall compared with the past due to strengthened prevention policies.
Southeast Asia shows wide variation from country to country. Some countries report relatively low official suicide rates, but this may reflect not necessarily lower actual risk, but rather the influence of cause-of-death classification systems, religious stigma, and underreporting. In rural areas, easy access to pesticides is also often identified as an important risk factor.
In South Asia, where the population is vast and the youth share is high, interpreting suicide statistics is especially important. In India and neighboring countries, large differences may appear by gender, age, and region, and household debt, agricultural crises, family conflict, youth unemployment, and women’s social vulnerability are often cited as major background factors.
To summarize the characteristics of Asia:
- East Asia: Strong influence of high-pressure social environments, aging, and urbanization
- Southeast Asia: Large country-to-country variation and strong effects from reporting differences
- South Asia: Youth, rural areas, and economic instability are important factors
- Some regions: Access to lethal means, especially pesticides, affects the statistics
Suicide Rate Trends in Europe
Europe is a region with relatively high-quality statistics, but there are clear differences within it among Western Europe, Eastern Europe, Northern Europe, and Southern Europe. Overall, many European countries have shown a long-term decline in suicide rates, though some countries still maintain high levels.
Western Europe often shows stable or declining trends over the long term, as mental health services are more accessible and social welfare systems are relatively well developed. However, new challenges also exist, such as urban isolation, the vulnerability of immigrant groups, and youth mental health problems.
Some countries in Eastern Europe and around the Baltic Sea have historically been known for relatively high suicide rates. In this region, socioeconomic instability after political transition, alcohol-related problems, differences in access to healthcare between regions, and male health vulnerability are often mentioned. Although some countries have recently seen declines, rates remain above the European average in some cases.
Northern Europe, despite its welfare-state image, does not always have low suicide rates. Overall welfare levels are high, but long-term mental illness burden, seasonal factors, feelings of isolation, and alcohol use problems can interact in complex ways. That said, this region has strong prevention systems and high-quality data, so policy responses are relatively systematic.
Southern Europe has traditionally been associated with strong family ties and relatively low suicide rates in some countries, but there have also been cases where risk increased among certain age groups after economic crises. Thus, even if cultural protective factors exist, they do not fully offset economic shocks.
Suicide Rate Trends in the Americas and Oceania
In the Americas, the differences between North America and Latin America are substantial, and Oceania also shows different patterns from country to country.
In North America, the United States and Canada are the main countries analyzed. Although these are high-income countries, it cannot be assumed that suicide rates are low. Access to firearms, drug addiction, limited healthcare access in rural areas, isolation among middle-aged men, and high risk in Indigenous communities are major issues. In particular, the United States shows very large disparities by region, race, and age.
In Latin America, many countries report relatively low or moderate suicide rates in official statistics, but there is considerable variation between countries. In some countries, family and community cohesion act as protective factors, while in others violence, poverty, youth unemployment, and a lack of mental health services increase risk. In places with incomplete reporting systems, rates may also be underestimated.
In Oceania, Australia and New Zealand are the main countries compared, and both have advanced mental health policies, yet the risk remains high in certain groups. In particular, suicide risk among Indigenous populations, rural residents, and young men is treated as an important public health issue. Pacific island countries have limited data, making accurate comparisons difficult.
Common factors in this region include the following:
- Wide regional disparities and rural vulnerability
- High risk among Indigenous and minority groups
- Effects of addiction, mental illness, and social isolation
- Differences in the quality of national statistics
Suicide Rate Trends in Africa and the Middle East
In Africa and the Middle East, it is important to consider limitations in statistical collection alongside the suicide rate itself. In many countries, death registration systems are not sufficiently developed, and because suicide is a highly sensitive religious, legal, and social issue, it may be underreported.
Africa varies greatly from country to country. Some countries show low official suicide rates, but this may be related not to low actual incidence, but to unregistered deaths, limited access to healthcare, and difficulties in determining causes of death. Many countries have a large youth population, and poverty, unemployment, conflict, forced displacement, and a lack of mental health services often interact.
In the Middle East, religious taboos and the possibility of legal punishment can affect suicide reporting. As a result, it is difficult to judge the true level of risk from official statistics alone. At the same time, war, refugee issues, political instability, youth unemployment, and social restrictions on women can all increase mental health burdens.
The following points are especially important when interpreting this region:
- A low official suicide rate does not necessarily mean low actual risk
- Weak death registration and cause-of-death classification systems are major variables
- Conflict, migration, poverty, and weak health infrastructure are difficult to reflect in the statistics
- Religious and cultural stigma makes reporting and research difficult
Main Causes of Regional Differences in Suicide Rates
Regional differences in suicide rates cannot be explained by a single factor. In general, economic conditions, mental health services, cultural attitudes, social safety nets, and access to lethal means are considered the key variables.
From an economic perspective, unemployment, income instability, debt, and recession can increase suicide risk. However, because high suicide rates can also appear in wealthy countries, national income alone cannot explain the issue. Even amid economic prosperity, competitive pressure, social isolation, and the burden of mental illness can grow.
Access to and quality of mental health services are also extremely important. Countries with strong systems for early diagnosis, counseling, crisis intervention, medication, and community-based support are more likely to reduce risk. By contrast, regions where stigma around mental health is strong or where there are too few specialists may respond too slowly in a crisis.
Culture and social structure also have a major impact. Family cohesion, community support, and religious norms can be protective factors, but they can also lead people to hide suicide attempts or mental illness, distorting the statistics. Structural issues such as gender-role expectations, pressure on men to suppress emotions, and women’s social dependence also affect risk.
In summary, the main causes are as follows:
- Economic instability: unemployment, poverty, debt, and regional inequality
- Healthcare system: access to mental health services, emergency response, and treatment linkage
- Social safety nets: welfare, unemployment protection, community care, and prevention of isolation
- Cultural factors: stigma, family structure, religion, and gender-role norms
- Access to means: availability of lethal means such as firearms, pesticides, and high-risk locations
Cautions and Implications When Looking at Suicide Rate Statistics
Suicide rate statistics are an important policy indicator, but they must be interpreted carefully. One of the biggest issues is differences in reporting standards across countries. Some countries have sophisticated systems for investigating causes of death and forensic analysis, while others are more likely to classify suicides as accidents or unknown causes. For that reason, simple cross-country ranking can lead to misunderstandings.
It is also risky to judge trends based on a single year’s data. In countries with small populations, even a small change in the number of suicide deaths can cause the suicide rate to fluctuate significantly. Therefore, it is better to look at multi-year averages, age-standardized figures, and detailed statistics by gender and age together.
From a policy perspective, attention should not be limited to countries with high suicide rates; it is also necessary to examine groups with rapidly increasing rates, specific regions or occupations, and high-risk groups such as young people, older adults, men, and Indigenous populations. Suicide prevention is not simply a medical issue, but a comprehensive challenge that includes education, labor, welfare, housing, and community networks.
Ultimately, suicide rate statistics mean more than just numbers. They signal how sensitively a society responds to mental health crises and how well it protects vulnerable people. When looking at the statistics, it is therefore more important to focus on understanding the context and the effectiveness of prevention policies than on competition over rankings.