Why HIV Prevalence Is So High in South Africa
Introduction: The Scale and Significance of HIV Prevalence in South Africa
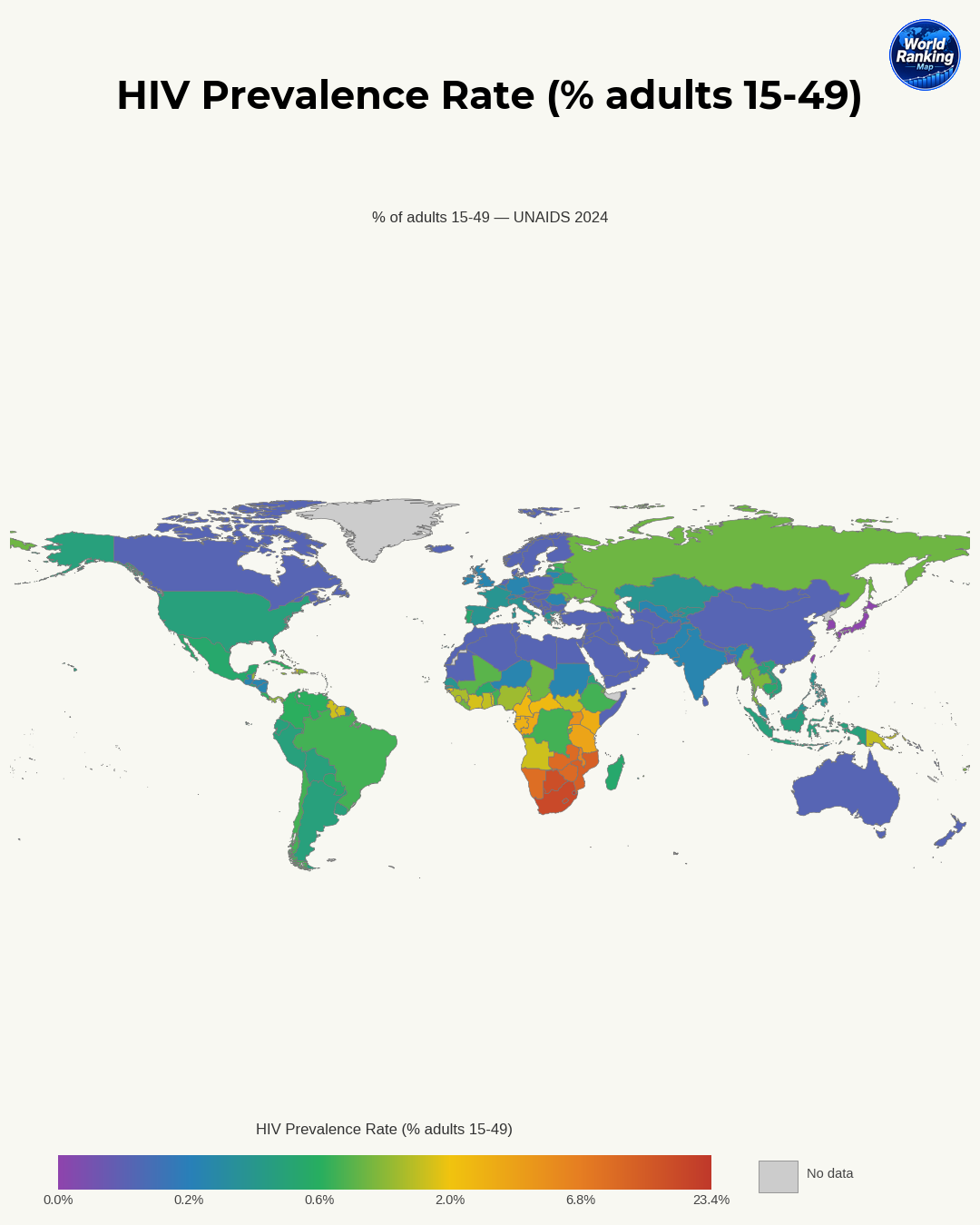
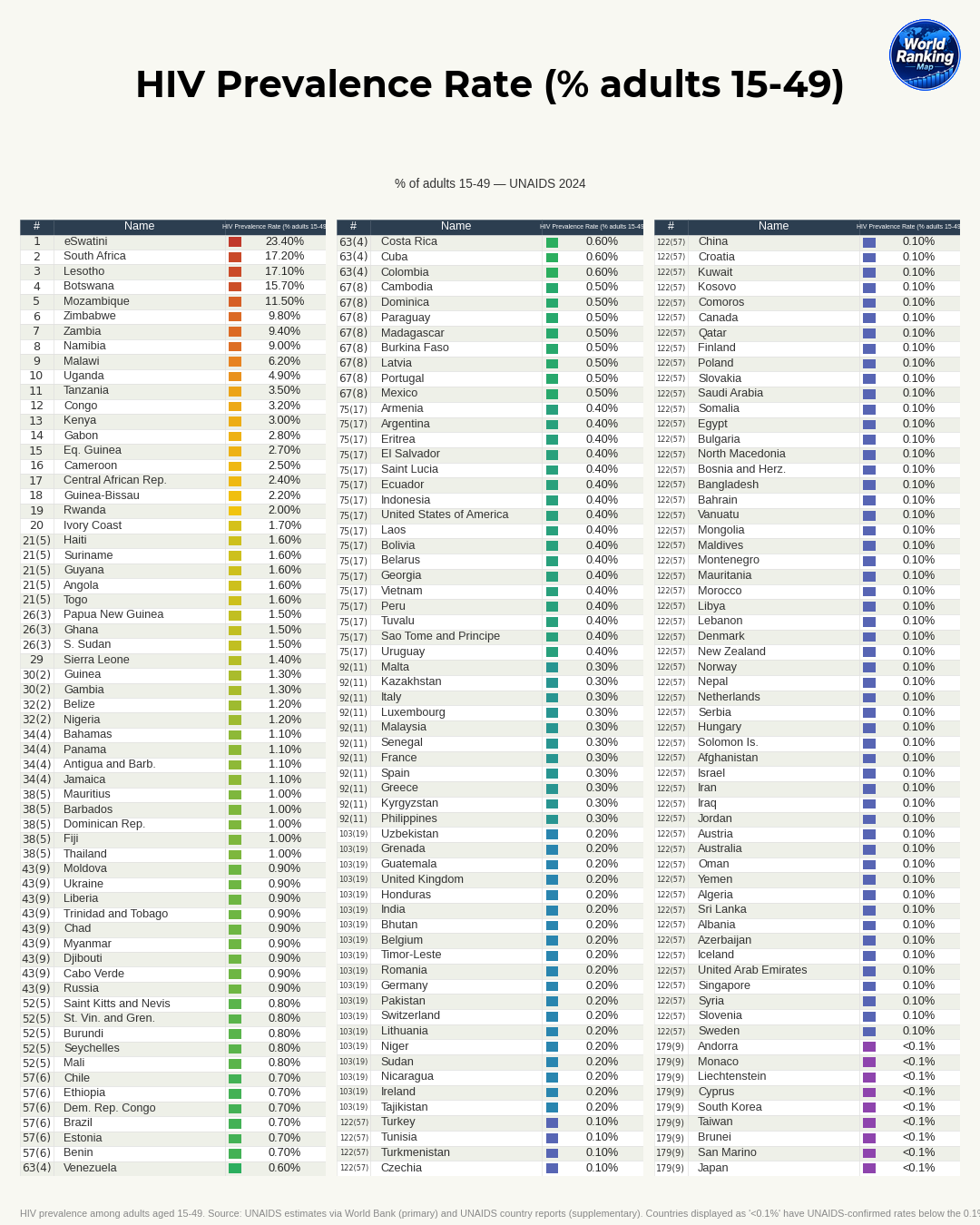
South Africa is regarded as one of the countries with the largest absolute number of people living with HIV in the world. Its prevalence among adults is also very high, making it a structural challenge that affects not only public health but also the labor market, household income, life expectancy, child welfare, and the national budget. HIV is now a chronic condition that can be managed with treatment, but unless the social conditions that concentrate infection are addressed, the epidemic will not easily decline.
To understand South Africa’s high HIV prevalence, we need to look not only at individual behavior but also at the intertwined background of history, the economy, gender relations, the health system, and community perceptions. This topic matters because South Africa is a leading example of how an infectious disease can become prolonged when it intersects with inequality.
Historical Background: The Spread of the Epidemic and the Limits of Early Response
South Africa’s HIV epidemic did not emerge overnight; it spread on top of the legacy of spatial segregation and social control during the apartheid era. Racial segregation policies confined the Black majority to poor residential areas and homelands, and created a system in which many male workers were sent for long periods to mines and urban industrial centers. In the process, a migrant labor system took root, and this helped expand sexual networks connecting different regions.
Rapid urbanization was another important factor. Informal settlements around cities had poor housing, sanitation, and access to healthcare, and social safety nets were weak. In such environments, prevention education, testing, and continuous treatment become difficult. An epidemic is not just a matter of a virus; it is also about the conditions under which people move and live.
The delay in the government’s early response also worsened the damage. In the 1990s and early 2000s, South Africa experienced political confusion and denialist messaging about the link between HIV and AIDS and the need for antiretroviral treatment. As a result, the expansion of testing and the introduction of treatment were delayed, and prevention of mother-to-child transmission did not move forward quickly enough. When an outbreak is not addressed aggressively at an early stage, transmission chains lengthen—and South Africa paid a heavy price for that.
Socioeconomic Factors: The Impact of Poverty, Inequality, and Unemployment
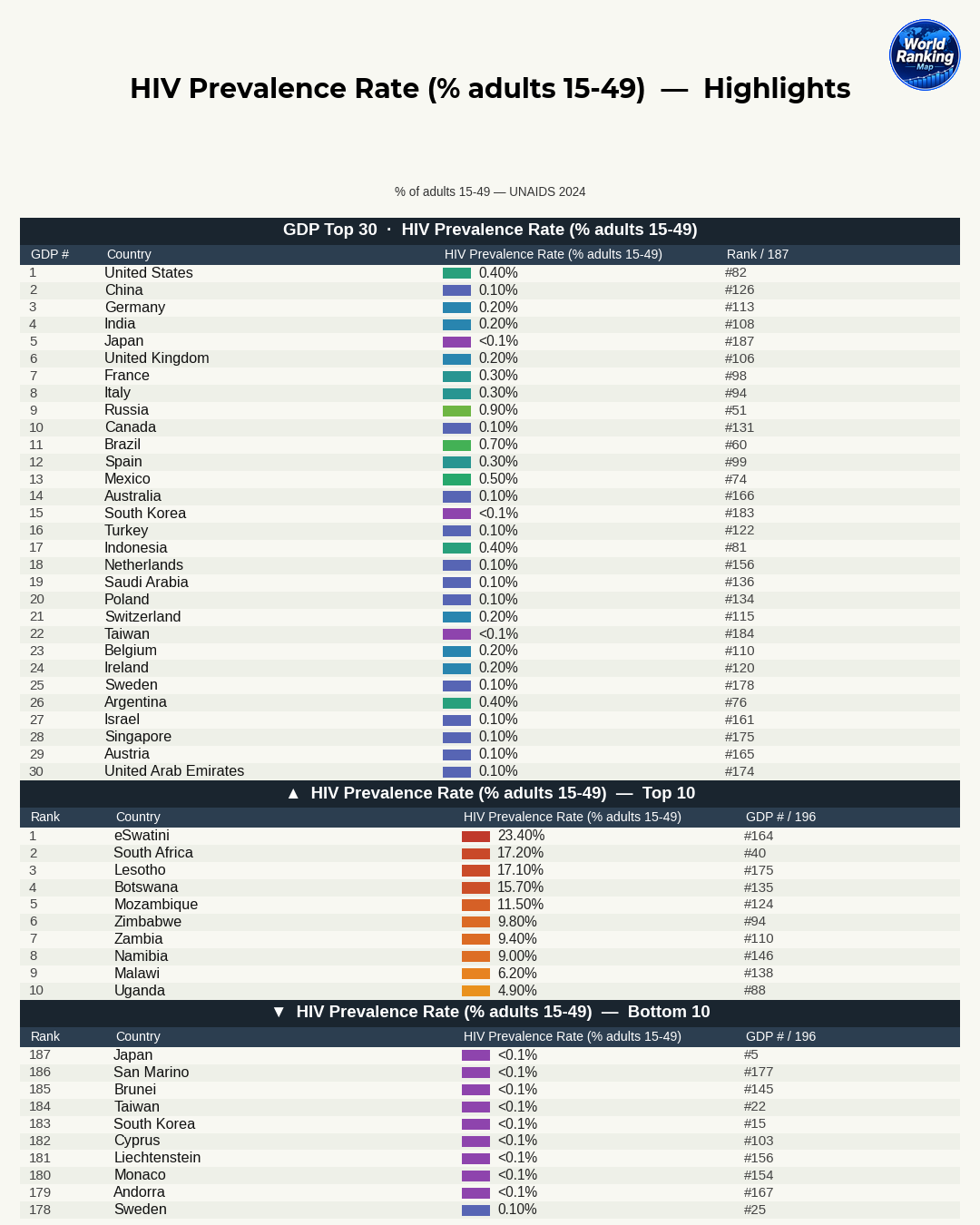
South Africa is also known globally as a country with very high income inequality. Even when GDP is high, if the benefits are not distributed evenly, many people still live with unstable housing, unemployment, and limited educational opportunities. These conditions directly hinder HIV prevention and management.
Poverty raises infection risk in several ways. People may delay testing because they cannot afford transportation, skip clinic visits because they need to work, or struggle to take medication consistently. Food insecurity also affects treatment adherence. Even when antiretroviral therapy is provided free or at low cost, the time and money needed to reach a clinic, and the opportunity cost of missing work, can make access much lower in practice.
In a society with high unemployment, young people are especially vulnerable. Economic dependence can weaken one’s bargaining power in risky sexual relationships, and some people end up in relationships based on financial support or survival needs. This makes it harder to use prevention methods and increases the likelihood of entering high-risk networks.
The key points are:
- Poverty reduces real access to testing and treatment.
- Inequality concentrates infection risk in specific regions and groups.
- Unemployment and precarious work make immediate survival take priority over prevention.
Gender Inequality and Gender-Based Violence
When explaining South Africa’s HIV epidemic, gender inequality is a central variable. Many women, especially young women, do not have enough bargaining power to insist on condom use or challenge a partner’s multiple relationships. When economic dependence, social norms, and the threat of violence combine, self-protection becomes extremely difficult.
Gender-based violence and sexual violence directly increase infection risk. Coerced sex can raise the likelihood of transmission through physical injury, and stigma and fear become barriers when survivors later try to get tested or treated. In violent relationships, even the use of prevention methods can become a source of conflict.
In South Africa, many studies also link relationships between young women and older men to higher infection risk. In relationships with large age gaps, economic and social power is often asymmetrical, and older men may already be part of broader sexual networks. In such cases, young women are more exposed to infection.
Ultimately, HIV is connected not only to biological factors but also to who holds decision-making power in relationships.
Challenges in the Health System and Education
South Africa has a relatively large health system by African standards, but there are major disparities in medical infrastructure across regions. Access to hospitals, staffing levels, and the speed of testing and referral can differ significantly between major cities and rural areas, and between affluent and poor communities. HIV requires early diagnosis and consistent treatment, and when that continuity is broken, it becomes difficult not only to protect individual health but also to suppress transmission in the community.
The quality and consistency of sex education are also issues. Even when HIV prevention is covered in schools, the information needed for real life—such as condom use, consent, healthy relationships, the need for testing, and the meaning of treatment—is not always fully conveyed. And even when people have information, stigma can prevent it from turning into action.
Stigma and discrimination remain powerful barriers. Fear that others will suspect them if they get tested, or worry that disclosure of their status could lead to disadvantages at work or in relationships, keeps many people outside the healthcare system. There is also the problem of loss to follow-up, where people are not immediately linked to treatment after testing or stop taking medication, which makes it harder to manage prevalence.
The main challenges are:
- Strengthening comprehensive sex education
- Expanding anti-stigma campaigns
- Improving immediate linkage from testing to treatment
- Reinforcing healthcare infrastructure in rural and low-income areas
Cultural and Behavioral Factors, and Community Perceptions
South Africa’s high HIV prevalence is also influenced by certain behavioral factors and social norms. These include multiple partnerships, concurrent relationships, reluctance to use condoms, and particular expectations around masculinity. The important point is that such behavior cannot be explained by individual choice alone; it is shaped by social norms and economic conditions.
In some communities, condom use is seen as a sign of distrust, or avoided because it is thought to reduce pleasure. And when traditional norms or religious beliefs clash with modern sexual health education, prevention messages may not be fully accepted.
Misconceptions and misinformation about HIV are also a problem. Beliefs such as thinking that treatment means there is no longer any need for caution, that it is a disease affecting only certain groups, or that folk remedies and unscientific treatments are sufficient can reduce prevention and treatment adherence. In societies with strong stigma, people are more likely to hide their status, which leads to delayed testing and continued transmission.
Improving community perceptions matters because HIV response does not happen only inside clinics. People are strongly influenced by messages from family, friends, religious communities, and local leaders.
The Role of Government Policy and International Support
After the delays in its earlier response, the South African government now runs one of the world’s largest antiretroviral treatment programs. This has made a major contribution to reducing mortality, restoring life expectancy, and lowering transmission through viral suppression. In particular, when people living with HIV receive treatment consistently and their viral load is suppressed, the chance of transmitting the virus to others drops sharply.
The expansion of prevention of mother-to-child transmission programs has also been an important achievement. With stronger testing and treatment during pregnancy, and better care before and after delivery, infant infections have fallen significantly compared with the past. This shows that policy intervention can genuinely change the course of an epidemic.
International support has also played a major role. PEPFAR, international organizations, and the Global Fund have supported testing, drug supply, healthcare worker training, data management, and community programs. Public campaigns have also achieved results in areas such as encouraging testing, distributing condoms, promoting male circumcision, and providing prevention education for young people.
But the limitations are clear.
- Even with expanded treatment, new infections have not been fully brought under control.
- Infection remains concentrated among high-risk groups, such as adolescent girls and residents of poor communities.
- Dependence on international aid can pose a challenge for long-term fiscal sustainability.
- Even with policies in place, uneven implementation and regional disparities can limit effectiveness.
In other words, South Africa has made clear progress in its HIV response, but it has not fully eliminated the structural causes of its high prevalence.
Conclusion: Key Priorities for Reducing High Prevalence
There is no single explanation for why HIV prevalence is so high in South Africa. Historical segregation and labor migration, extreme inequality, gender-based violence, unequal access to healthcare, stigma, and behavioral and normative factors have combined over a long period to create the current situation. The solution, therefore, cannot be singular either.
The priorities ahead are clear. First, prevention must be strengthened. Comprehensive sex education, condom access, and prevention strategies for high-risk groups need to be more tightly woven together. Second, early diagnosis and immediate linkage to treatment must improve. Third, people who start treatment need support to continue it over the long term so they do not drop out. Fourth, to protect young women and vulnerable children and adolescents, women’s economic and social empowerment and violence prevention are essential. Fifth, and most fundamentally, poverty and inequality must be reduced in parallel.
South Africa’s experience shows that HIV is not just a medical issue, but a mirror reflecting the structure of society as a whole. Reducing high prevalence requires more than medicine alone; it requires a fairer society and a more accessible health system working together.